Historical Metal-on-Metal THR's
Hip resurfacing has always been an attractive concept and the theoretical advantages of hip resurfacings are:
- Minimal bone resection
- Normal femoral loading
- Avoidance of stress shielding
- Maximum proprioceptive feedback
- Minimal risk of dislocation
- Easy revision
- Restores normal anatomy:
- Offset
- Leg length
- Anteversion
Sir John Charnley carried out the first hip resurfacing in the 1950's using Teflon on Teflon bearings but unfortunately these Teflon bearings wore out within two years. This problem of failure of hip resurfacing materials was to plague surgeons and engineers for the following thirty years. The 1970's saw the next significant development of hip resurfacing using materials available for total hip replacement of the day.

Freeman36 and Furuya37 performed hip resurfacing using polyethylene femoral components and metal acetabular components.

Due to excess wear they, Wagner38 and Amstutz39 all converted to metal heads against polyethylene acetabular components with all components fixed with poly-methylmethacrylate cement.

The Wagner resurfacing arthroplasty was used in Birmingham in both its metal on polyethylene and ceramic on polyethylene forms, but the results were very disappointing and show a 55% failure rate at 6-7 years.

The particular problems with the Wagner were loosening of components and collapse of the femoral head and these extremely disappointing results in the hands of many surgeons encouraged the view that the concept of hip resurfacing arthroplasty was flawed. However, closer examination of the failure patterns show that this was a failure of materials rather than a failure of concept.40
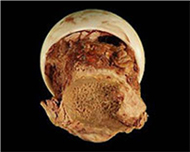 |
The ceramic Wagner femoral component shown at left was resected from a patient whose cup loosened at nine years and the femoral component was solid. |
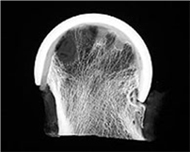 |
This was prepared by Professor Archie Malcolm's laboratory in Newcasde upon Tyne. Micro-radiography of the sliced specimen shows trabeculae streaming down from the cement plugs but worryingly holes are present in the substance of the femoral head. |
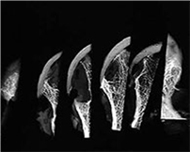 |
Other slices of the femoral head also show marked cavitary defects. |
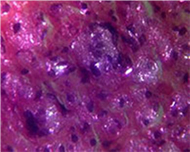 |
Histology in the areas of bone loss shows macrophages laden with polyethylene debris. |
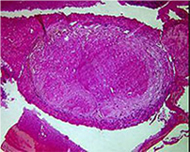 |
Granulomata were present on every slice of the femoral head. |
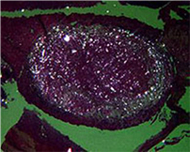 |
On polarised light microscopy, the granulomata are seen to be full of polyethylene debris. This shows clearly that the erosive process in the femoral head is a result of polyethylene debris osteolysis. |
If we consider the situation of hemi-resurfacing arthroplasty, which is performed in avascular necrosis patients with intact acetabular cartilage, then we can see the normal outcome of a cement-fixed femoral resurfacing shell in the absence of polyethylene debris. Long term results show that these herni-arthroplasties do not fail by collapse of the femoral head and Grecula et al. report a zero loosening rate of these hemi-resurfacing arthroplasties at 15 years.41
End of the First Era of Resurfacing
The conclusion of the 1970's and 1980's experiment with hip resurfacing was that:
THE BAD RESULTS OF RESURFACING
WERE
THE RESULT OF BAD RESURFACINGS.
It was clear that polyethylene could not be used as the bearing material in hip resurfacing as the inevitable use of a large femoral head size in the resurfacing arthroplasty would lead to excess polyethylene debris, osteolysis, loosening and collapse of femoral heads. A bearing material had to be found which would be durable for use in young active patients, and would be durable when used with a large diameter articulation. In addition, the bearing material had to be capable of manufacture as a thin component to avoid excessive resection of valuable bone stock in young patients. Ironically such material had in fact been in successful clinical use for thirty years but had not been used in resurfacing arthroplasty in any significantly large study.
© 2007 Smith & Nephew